


Patients with multi-directional instability are often successfully treated with conservative measures. The mainstay of treatment is a comprehensive shoulder and periscapular rehabilitation program emphasizing strength and proprioceptive training. For a small group of patients who continue to have an unacceptable degree of instability that interferes with their preferred activities and who have had extensive physical...

There is considerable variability among people in terms of their shoulder anatomy and function. Because of this, we all find ourselves somewhere on the spectrum of shoulder stability. On one extreme, we find people with “tight” shoulders that are highly resistant to dislocating, but with limited shoulder motion and often some degree of pain, depending on their activities. On the other extreme, we find people with “loose,” highly mobile, unstable shoulders, some...
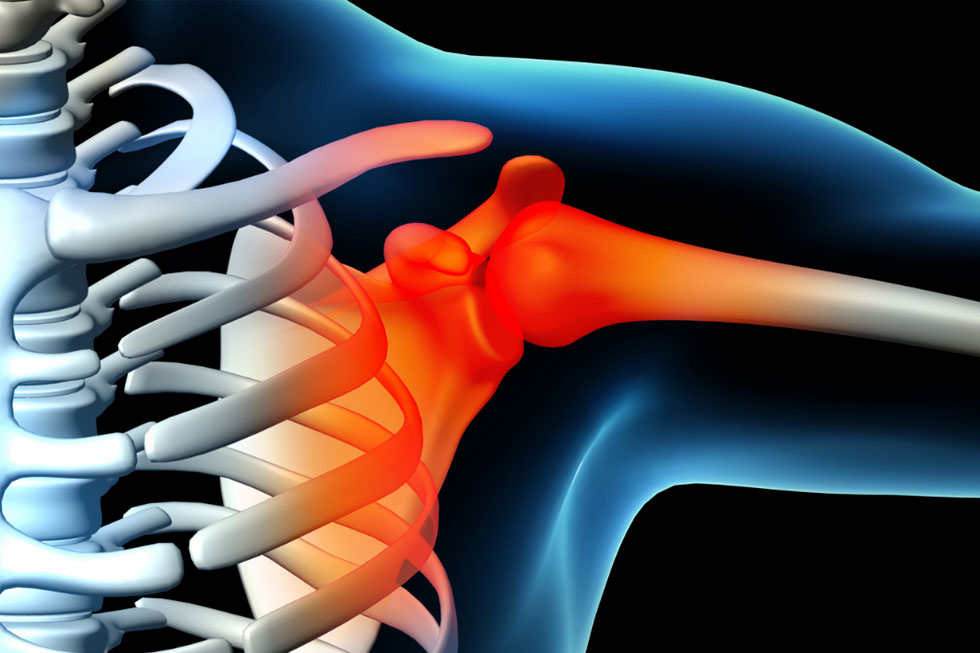
The main “ball and socket” joint of the shoulder (the glenohumeral joint) is formed between the relatively small, shallow socket of the shoulder blade (the scapula) and the large ball of the upper arm bone (the humerus), much like a golf ball balancing on a golf tee. This relationship allows for a highly mobile joint, but one that is, unfortunately, not well-stabilized by the bones alone. Therefore, the surrounding soft tissue...