


Understanding the nuances between different squat variations can significantly impact your training journey. Whether you’re looking to train around pain, choose a squat style that complements your body type, or simply crush your fitness goals, knowing the pros and cons of each squat can be a game-changer. Front Squat, Back Squat, and Low Bar Back Squat, and discover which one aligns with your training objectives...

Dr. Nels Sampatacos discusses his approach to cartilage transplant surgery with Connor Bevans, the Arthrex and Summit Surgical Orthobiologics Specialist for Western Washington podcast...

Most studies report good to excellent results after SLAP repairs in 84-97% of patients.5-7 However, some patients may not do as well with a SLAP repair, particularly those with biceps tendinitis or partial tearing of the biceps tendon.8 In these cases, treatment of a SLAP tear may necessitate detachment of the biceps tendon from the torn superior labrum. This can be done in several...

Accurate diagnosis of SLAP lesions often requires an MRI with a special contrast injected into the joint. Although the literature is variable, most studies show that a conventional MRI allows for the detection of labral injuries only 26-62% of the time. When contrast is added, our ability to diagnose these injuries increases to over 90%...

Superior Labrum Anterior and Posterior (SLAP) lesions describe a spectrum of injuries to the superior portion of the labrum, where one of the two biceps tendons partially attaches. The labrum is a bumper with a rubber-like consistency that surrounds the socket (i.e. glenoid) of the shoulder. It provides stability to the shoulder and is an important attachment site for the biceps tendon and other shoulder ligaments...

Nonsurgical management is the treatment of choice for grades I and II AC separations. This consists of wearing a sling for 1-2 weeks, at which time patients with grade I injuries can return to full activities as pain allows. Grade II injuries often require physical therapy and avoidance of sports and heavy lifting for at least 6 weeks. Persistent pain is often minimal in the short-term, although up to 50% of grade I and II injuries develop pain...
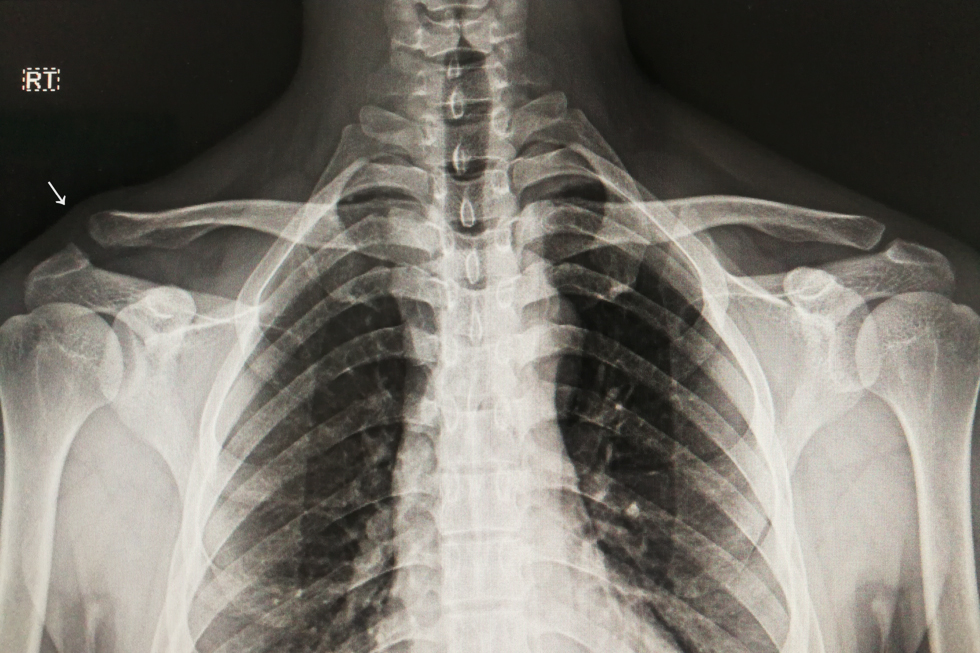
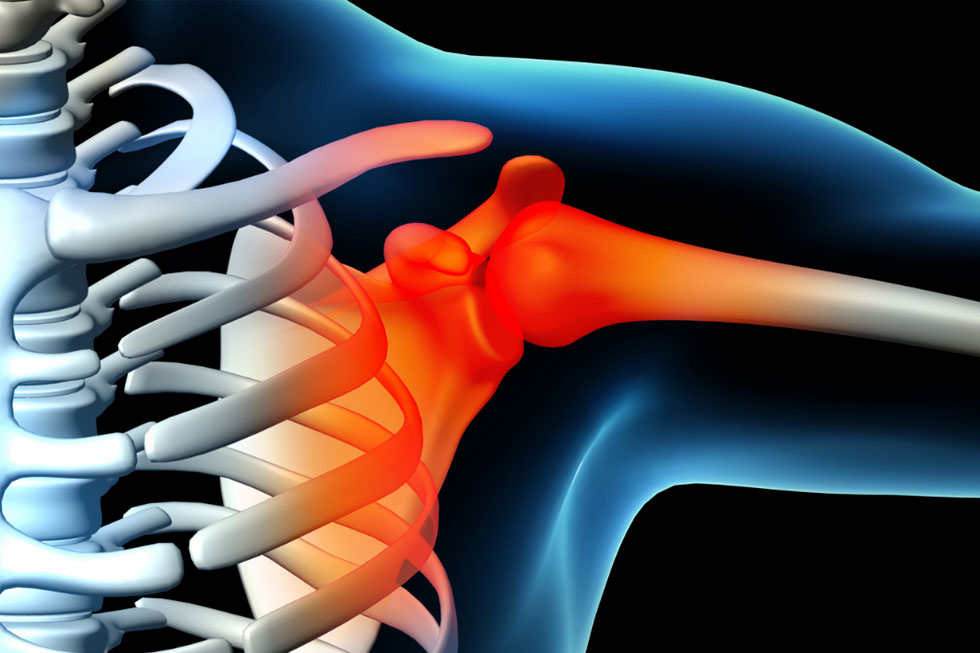
There are a number of muscles, tendons, and ligaments attaching to the bones of the shoulder (e.g. the scapula, humerus, and clavicle) that maintain the bones in a normal position to one another. The acromioclavicular (AC) joint is the joint between the acromion (part of the scapula) and the end of the clavicle (collar bone). The AC joint is normally stabilized by the AC joint capsule...

Patients with multi-directional instability are often successfully treated with conservative measures. The mainstay of treatment is a comprehensive shoulder and periscapular rehabilitation program emphasizing strength and proprioceptive training. For a small group of patients who continue to have an unacceptable degree of instability that interferes with their preferred activities and who have had extensive physical...

One general category of shoulder instability typically involves a traumatic event in an individual with normal tissue elasticity, resulting in a single-direction dislocation and tearing of soft tissue structures. This is particularly common in younger patients and is often treated with surgery. For example, in the most common scenario, the ball dislocates in an anteroinferior direction, resulting in tearing of the anteroinferior portion...

There is considerable variability among people in terms of their shoulder anatomy and function. Because of this, we all find ourselves somewhere on the spectrum of shoulder stability. On one extreme, we find people with “tight” shoulders that are highly resistant to dislocating, but with limited shoulder motion and often some degree of pain, depending on their activities. On the other extreme, we find people with “loose,” highly mobile, unstable shoulders, some...
The main “ball and socket” joint of the shoulder (the glenohumeral joint) is formed between the relatively small, shallow socket of the shoulder blade (the scapula) and the large ball of the upper arm bone (the humerus), much like a golf ball balancing on a golf tee. This relationship allows for a highly mobile joint, but one that is, unfortunately, not well-stabilized by the bones alone. Therefore, the surrounding soft tissue...

Meniscus tears are commonly diagnosed and treated with physical therapy, chiropractic, and massage. The size and location of the tear will influence the likelihood of recovery. When treating these tears, our main rehabilitation goals include: restoring pain free range of motion, strengthening the muscles and connective tissue around the knee, identifying weak links at other locations in the body, and improving movement patterns that may cause excessive loading on the knee.
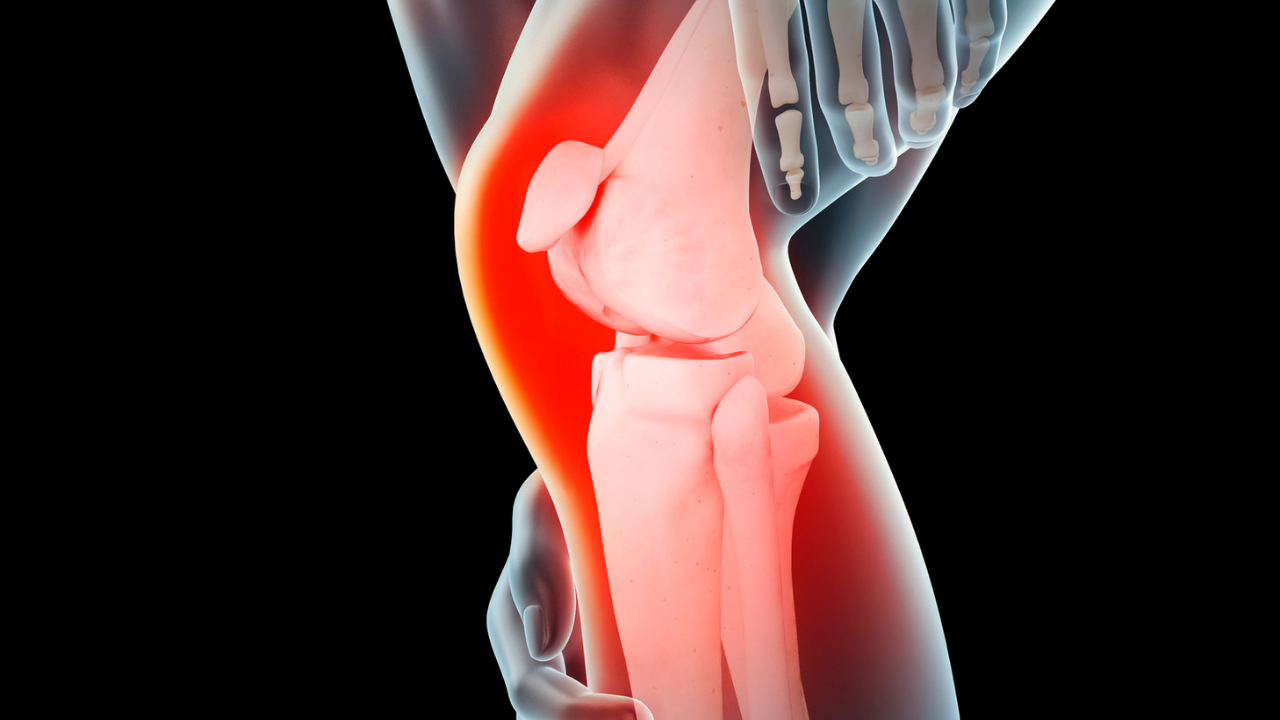
The anterior cruciate ligament (ACL) is one of the four primary stabilizing ligament complexes of the knee and plays an important role in activities that involve cutting and pivoting movements. There is a spectrum of injury patterns that can affect the ACL ranging from partial to complete tears. Furthermore, concomitant injuries occur in nearly 50% of cases and may include the cartilage surfaces, other knee ligament...